- A
- A
- A
- ABC
- ABC
- ABC
- А
- А
- А
- А
- А
Mortality from COVID-19
© ISTOCK
A major public debate has erupted over numerous articles in foreign and Russian media about the ‘Russian miracle’ and the ‘riddle’ of how the coronavirus has behaved in Russia, compounded by the admission by the Health Minister of the Republic of Dagestan concerning the ratio of coronavirus deaths to so-called ‘community-acquired pneumonia.’ How reliable is the data collected by Russia’s official agencies? Can the authorities rely on them when making decisions? Which two types of statistics should be used during an epidemic? Demographers Sergey Timonin and Anatoly Vishnevsky answer these and many other questions.
Sergey Timonin,
Deputy Head,
International Laboratory for Population and Health,
HSE
Anatoly Vishnevsky,
Director Institute of Demography, HSE
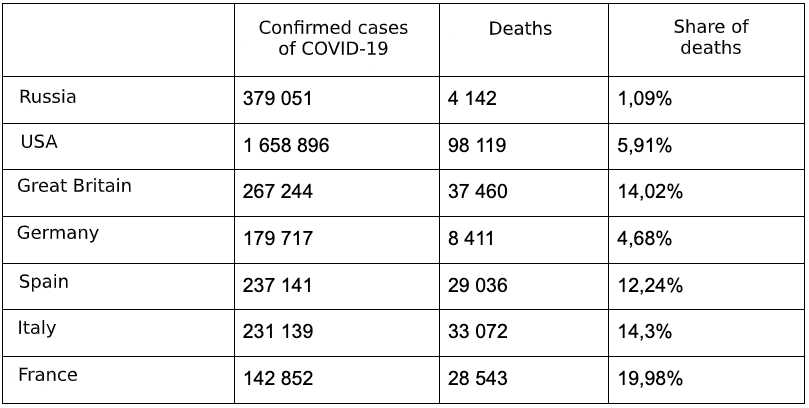
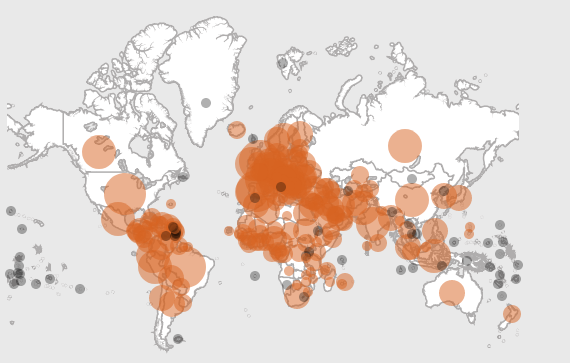
According to a World Health Organization (WHO) report based on data obtained from official national sources, Russia had registered 379,000 confirmed cases of COVID-19 infection on May 28. Of those, 4,100 (1.09%) ended in death. When comparing these data with statistics from other countries, Russia’s exceptionally low coronavirus mortality rate — that is many times lower than what some other states have experienced — stands out and raises unavoidable questions.
{kind=link}
What is the reason for these differences? Do they reflect the true state of affairs or are they attributable to Russia’s outmoded methods for publishing statistics? The answers to these questions largely determine the policy the authorities adopt for combatting the pandemic.
Can we compare COVID-19 mortality rates using current country estimates?
Traditionally, official agencies base their cause of death statistics on information obtained from medical death certificates. These certificates are filled out in accordance with generally accepted rules that were adopted at the international level more than 70 years ago. If the death certificate indicates several causes, one is identified as the first and main cause that set off the chain of maladies that ultimately ended in death. In this case, all other ailments are considered complications of the main illness or as contributing to it (comorbid).
Cause-of-death statistics are based on the original cause. Even under ‘normal’ conditions, identifying the primary cause can be a somewhat subjective and weighty task. The COVID-19 pandemic, that poses the greatest threat to elderly people with severe comorbidities, creates additional difficulties in identifying the original cause of death.
As soon as SARS-CoV-2 began spreading beyond China, most countries of the world began publishing key indicators that would make it possible to monitor how the epidemic was progressing within their borders. However, the standard rules for such reporting were not designed for use during a pandemic, and because countries interpreted them differently, it led to inconsistencies in the information they published. Moreover, because countries take different approaches to determine which deaths were caused primarily by COVID-19, it was inevitable that discrepancies would arise between their respective mortality statistics.
When deciding which cases should be included in their COVID-19 mortality statistics, some countries counted the deaths of all people diagnosed with the new coronavirus, regardless of the degree of severity. Others reported only the number of COVID-19 patients who died in hospitals. Many countries, such as Great Britain, did not initially include the deaths of nursing home patients because they are non-medical facilities and report to a different government agency. A third group of countries adopted narrower criteria, limiting the number of deaths to those where the coronavirus infection was the main cause of death.
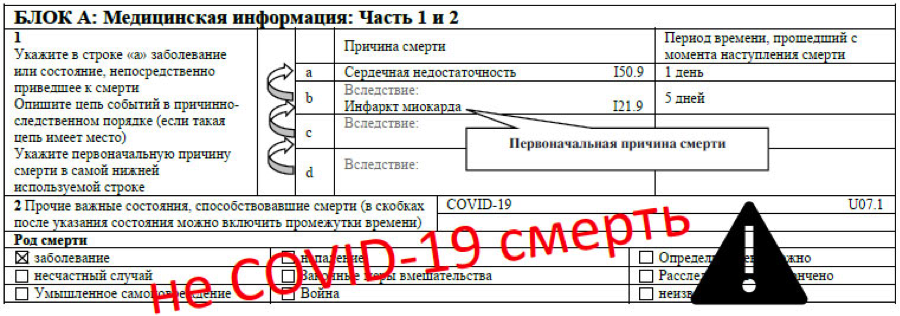
What's more, the WHO did not provide clear guidance on this issue. When introducing its emergency codes for COVID-19 (U07.1 and U07.2), WHO stated that ‘the rules for selecting the initial cause of death are the same as for influenza’ and ‘no additional guidelines are required for filling out a medical death certificate.’ On April 16, 2020, however, WHO released the document ‘International guidelines for certification and classification (coding) of COVID-19 as cause of death’ instructing that ‘COVID-19 should be recorded on the medical certificate of cause of death for ALL decedents where the disease caused, or is assumed to have caused, or contributed to death.’
On the one hand, the ‘Recommendations’ section of that document clearly states: ‘A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19.’ On the other hand, ‘Persons with COVID-19 may die of other diseases or accidents, such cases are not deaths due to COVID-19 and should not be certified as such.’ It then gives examples in which the original cause of death is a different disease (such as myocardial infarction) and COVID-19 is considered a contributing cause (comorbid disease), with the result that ‘the death may have been influenced by COVID-19, but death was caused by another disease or an accident.’
{kind=link}
One thing is clear: WHO insists that COVID-19 should always be listed in one of the columns of the medical certificate of death, as either the original or an underlying cause of death.
At the same, there was a growing understanding that during an epidemic, it was necessary to track all deaths associated with the presence of COVID-19. This was true regardless of whether the coronavirus infection started a chain of pathological changes in the person’s body that led to death or appeared later in such a chain started by another cause, and only accelerated the person’s death.
This understanding is important not only for the medical community to fulfil its professional duty but also for society as a whole. After all, a pandemic brings a much greater risk of poor health and death than is present during normal ‘peaceful’ conditions. This is why the discussion of how to record the cause of death in a pandemic went beyond the scientific community and resonated with the public.
Consider, for example, the White House briefing on April 7, 2020 that featured, in addition to U.S. President Donald Trump making his usual statements, an explanation by Deborah Birx — who has served as Global AIDS Coordinator for Presidents Barack Obama and Trump, and as Trump’s Coronavirus Response Coordinator. She said that although some countries attribute the cause of death to pre-existing conditions that were exacerbated by the coronavirus, ‘Right now, we’re still recording it, and…the intent is, right now…if someone dies with COVID-19, we are counting that as a COVID-19 death.’ It was apparently no accident that she used the words ‘right now’ twice in the same sentence.
White House briefing, April 7, 2020
In addition, every week the Center for Disease Control and Prevention (CDC) publishes and updates data on deaths from COVID-19, pneumonia and flu based on information gleaned from death certificates. What's more, the CDC includes not only the total deaths in which COVID-19 was the original cause but also those in which the coronavirus infection acted as a catalyst — although those cases represent only 6% of the total, as indicated by U.S. death certificates.
How does Russia currently gather information about COVID-19 deaths?
In accordance with the temporary guidelines of the Russian Health Ministry, every patient who dies with a confirmed or suspected diagnosis of COVID-19 must undergo a post-mortem examination. Based on the results of the autopsy (including histological examination of organs and analysis of autopsy material for the presence of viral and bacterial pathogens), a final pathological diagnosis is made in accordance with the Russian Society of Pathologists’ clinical guidelines contained in its document ‘Formulation of pathoanatomical diagnosis in some infectious and parasitic diseases.’
If the doctor who conducted the autopsy definitely determines that COVID-19 was the primary cause of death, it will be listed as such on the death certificate. If, however, the clinical and morphological evidence indicates another ailment such as injury or poisoning was the primary cause, that will be reflected on the death certificate. In this case, the new coronavirus infection will be listed as a comorbid or contributing cause of death.
If COVID-19 is recognized as a comorbid disease (most often combined), then the death is listed as resulting from other pre-existing serious illnesses, the exacerbation or adverse course of which was caused by the ‘addition’ of the coronavirus infection. In such situations, COVID-19 must be listed on the medical death certificate as ‘another important condition that contributed to death’ (see the Moscow Health Department Interim Guidelines).
What coronavirus symptoms look like, day by day
If a death occurred ‘due to various life-threatening diseases and their complications in the absence of clinical manifestations and pathological changes caused by the SARS-CoV-2 virus,’ but a laboratory has confirmed the presence of the virus, then COVID-19 is a ‘co-existing disease’ that did not contribute to death and is not listed in the medical certificate of death.
The Russian recommendations are generally consistent with the WHO guidelines for determining COVID-19 as the cause of death, but they do not answer the question of what picture Russia’s current statistics convey — a picture that serves as the basis of operational decisions by Russian authorities. It seems that these statistics do not include all deaths involving COVID-19, unlike the practice of the U.S., for example.
In all likelihood, the Russian statistics include only those cases in which COVID-19 was the main or original cause of death. An analysis of data from certain regions confirms this. For example, the portal for Chelyabinsk lists information about both ‘death from COVID-19’ (16 cases on May 29, 2020) and of deaths in which COVID-19 was a ‘comorbid disease’ (21 cases on May 29, 2020). The federal level, however, lists only 16 deaths in the Chelyabinsk region — that is, only those in which COVID-19 was the primary disease.
A statement by the Moscow Health Department on May 13, 2020 indicates, for example, that ‘post-mortem diagnoses and causes of death are, in the end, extremely accurate… It is impossible to name COVID-19 the cause of death in other cases. Thus, for example, more than 60% of deaths resulted from clearly alternative causes.’ This is one more proof that only those cases in which COVID-19 was the main or original cause of death were included in the official count.
What should cause-of-death statistics look like during an epidemic?
The generally accepted principle of reporting cause-of-death statistics has been developed over the course of many decades and the crisis caused by the pandemic should not call it into question. That principle stipulates the identification of one original cause of death among the diseases present, with the remainder to be listed as comorbidities or complications of the underlying disease. This is extremely important even under 'normal' conditions when efforts by healthcare workers are focused on fighting non-communicable chronic illnesses.
If to abandon that and shift the center of gravity to the immediate or comorbid cause of death, the resulting increase in mortality from, say, flu, could create the illusion of decreased mortality from, for example, cardiovascular diseases. In fact, not only does the contributing role they play in death not weaken, but actually increases due to the additional influence of an infectious agent — that would not be nearly as dangerous for a healthy individual. On the other hand, under-reporting the role of flu or the new coronavirus infection in tanatogenesis might create the illusion that the epidemic is not serious and lead to an unjustified statistical increase in mortality from chronic diseases.
{kind=link}
Furthermore, in the current epidemic, some of the ‘excess’ deaths from certain diseases might not only be connected to the infectious agent, but could also be caused by the quarantine measures and their consequences. For this reason, it is important to separate deaths directly related to COVID-19 from those with only an indirect connection to it.
Thus, cause-of-death statistics based on the identification of the original cause of death hold fundamental importance and are necessary for addressing the long-term challenges facing society and the healthcare system. This does not exclude the possibility, however, that under certain conditions society might need knowledge and a different set of statistics. This can happen when an epidemic first appears and urgent, ‘targeted’ measures are required to prevent it from spreading.
In this situation, information is needed on all deaths associated with the disease responsible for this epidemic, regardless of whether it was the main cause or simply one link in the chain of health disorders that led to death. That means we need to produce two sets of interconnected data — one for meeting long-term objectives under ‘normal’ conditions, and a second for mounting an emergency response to the epidemic and preventing new outbreaks.
If no second set of data exists, the statistics ‘don’t see’ the actual causes of death, making it necessary to assemble that picture later, after everything has ended. By way of illustration, consider the 2016-2017 flu epidemic in England in which the authorities issued fewer than 1,000 medical death certificates mentioning the flu. According to an assessment conducted later by Public Health England, an average estimate revealed that the number of flu-related deaths that season was actually 18 times higher.
This type of more or less accurate estimate can be made post factum, when the total number of deaths from all causes is known and can be compared with the usual total in years without an epidemic. That is important for understanding long-term trends, for developing preventative measures and so on, but it is useless for mounting a rapid response.
Can Russian statistics provide two sets of cause-of-death data?
Russian statistics can collect this information in two ways. The first is to indicate COVID-19 on the death certificate ‘across the board’ — that is, not only when it is the main cause of death, but also when it is a comorbidity. This would enable the State Statistics Service to provide statistics reflecting both realities.
The federal registry of persons infected with the new coronavirus could provide an additional and more complete source of information about COVID-19-related deaths. If the instructions posted on the Health Ministry’s portal are followed, then all patients with COVID-19 should be included in the registry.
In the event one of those patients dies, information about the preliminary and final pathoanatomic/forensic diagnosis, as well as codes for the causes of death listed on the death certificate should be entered in the registry. Thoroughly and properly entering the required information in this registry makes it possible not only to collect the data needed for a comprehensive analysis of all COVID-related deaths, but also to later help develop Russia’s final cause-of-death statistics and to conduct scientific research.
IQ